
How Might We Empower Students to Find Reliable, Accessible Sexual Health Resources?

by Julienne Ho, James Lucassen, Max Hui, and McKenna Blinman
Content warning: mentions of sexual assault
Note: names of interviewees are changed to protect their privacy
This summer, our team of four 5C students had the privilege of participating in the Summer Fellowship run by the Hive. The prompt of the fellowship challenged us to dive deeply into problems surrounding wellness on the Claremont Colleges’ campuses, especially as students return from our COVID-19 lockdowns. Seeing an opportunity to further develop a previous design project surrounding sexual health, Julienne assembled a team to tackle the challenge. McKenna, Max, and James were all on board.
Our previous research, which involved a first round of interviews, had honed in on one particular point of view (POV) from an impactful interview: Marcy. On the day after having sex in which the condom broke, she is unsure of what to do. She has a physics midterm in three hours, so she has to decide whether or not to commute to the nearest Target for Plan B and risk missing the beginning of the test, when the doors are locked to prevent distractions for the test-takers. Marcy is aware that the efficacy of Plan B diminishes as time after fertilization increases. Unable to access a solution last night, because stores were closed, she is now overwhelmed with an impossible decision: should she risk failing physics, or should she risk becoming pregnant?
At the start of this fellowship, we decided to conduct a second round of interviews. With ten additional perspectives on sexual health on campus, we understood that the most time-sensitive, panic-inducing experiences involved pregnancy scares. Our secondary research from literature review on the subject revealed that pregnancy scares are distressingly common among college-aged students. While statistics on the prevalence of pregnancy scares vary due to a variety of factors, a study by the National Institute of Health using a random, population-based sample of women aged 18-19 found that 33% of them experienced a pregnancy scare over the two years when the study took place (Gatny et al, 2018).
From our interviews, we inferred that accessibility to necessary sexual health resources was the driving factor behind the majority of our interviewees’ stress during pregnancy scares. At up to $70, as one student cited, emergency contraception can be cost-prohibitive. The physical distance needed to obtain the drug created temporal restrictions which conflicted with students’ schedules, like Marcy experienced. The most commonly cited inconvenience among our interviewees, across all campuses and age groups, was accessibility at night. Students tend to be more sexually active at night, and demand for sexual health products consequently skyrocket while businesses are closed.
The second interview that stood out to us most was with Jess, a first-year college student who was pressured into having sex without a condom. Her regular hookup, whom she’d been seeing for months, had betrayed her trust. Feeling hurt, violated, and overwhelmed, she isn’t sure what to do. Jess is aware of the Plan B vending machine in Walker Lounge on the Pomona campus, but she does not have swipe access to that building as a Scripps student. As a first year student, she does not have the deeper trusting relationship with someone off-campus that would be necessary in order for her to feel comfortable divulging this sensitive information. She feels ashamed and does not wish to justify why she relented to unprotected sex, especially to an acquaintance who might not understand the complicated emotions and pressure associated with her experience. She wishes she could instantly and anonymously get emergency contraception in order to stop panicking about the night before.
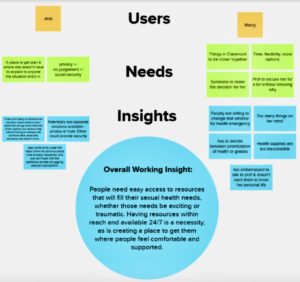
Our guiding problem statement, synthesizing these various interviews, was “How might we empower students to find reliable, accessible sexual health resources?”
With this, we launched into our ideation phase, generating hundreds of ideas.

In order to build upon these ideas, we did a “yes, and” activity. Following this, we each picked several favorites. We mapped these favorites onto 2×2 grids weighing our top four criteria for selection: cost-effectiveness, anonymity, likelihood of implementation, and independence from school administration infrastructure.
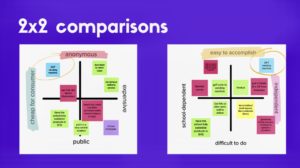
One option stood out clearly to us: an anonymous vending machine that is open 24/7. With this choice of solution, we launched ourselves into a testing phase.
Our next step was to seek out user feedback with a survey, to help us iterate on this idea and make various trade-offs during the design process. Of the questions we asked, three produced particularly useful results that ended up significantly influencing the development of our prototype. The first of these questions was about the trade-off between offering anonymity and human comfort – we asked whether our users would be more comfortable buying sexual health products from a human, from a machine, whether they were indifferent, or wouldn’t buy these products at all. These were the results:
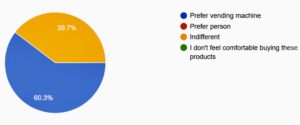
Out of the 63 responses we received, most preferred a vending machine and not a single one preferred the human option! We incorporated this valuable information into our prototyping process by focusing on automatic, anonymous solutions. The next trade-off we faced was between a uniform design or a unique one. We asked users to rate on a scale from 1 to 5 whether they would prefer something uniform (1) or creative (5). These were the results:
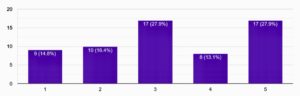
We saw that our users leaned in the direction of creativity, but not too drastically. Our goals for this design specifically included improving accessibility and making sure the result worked for everyone, so we listened to this feedback and decided to be creative with the design. At the same time, we wanted to keep things anonymous to make sure those that prefer a more discreet solution would still be comfortable. The last question we iterated on was about the trade-off between accessibility and privacy. We asked our respondents to rate on a scale from 1 to 7 how important it was for the location to be near them, and these were our results:
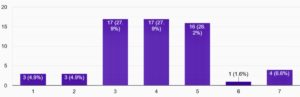
This tells us that almost all of our users do care about distance somewhat, but not overwhelmingly so. From this, we were able to conclude that our users largely preferred a middle ground between a location in some obscure, private corner of campus and a highly distributed, extremely local solution. As a result, we decided on having a single centralized location near the center of campus, such as the Student Health Services building.
With this prototype ready for implementation, all that remains is to make it a reality. In the coming weeks and after we return to campus, we will be sourcing the vending machine itself, coordinating with students and administration to help the machine become operational and self-sustaining, and conducting an outreach campaign to kickstart the effectiveness of our solution. We hope that this will allow the machine to start improving the lives of students right away by providing better healthcare options with anonymous access and accompanied by educational resources and a support/feedback system. We hope that in the long run our solution will no longer have to be novel to garner attention but simply a fact of campus life, widely known to the student body and available to all students, at all schools, at all times. Finally, we hope that its influence will help shift the culture surrounding sexual health on campus by making it more accessible, safe, and informed.
Gatny, Heather et al. “Pregnancy scares and change in contraceptive use.” Contraception vol. 98,4 (2018): 260-265. doi:10.1016/j.contraception.2018.07.134
Summer Hours
Mon – Thurs | 9am – 4:30pm
Friday | 9am – 3pm
Weekends | Closed
